NIR-T/BSS
Near InfraRed Transillumination with Back-Scattering Sounding.
Method explained by Andrzej F FRYDRYCHOWSKI, M.D., Ph.D, Prof.:
The concept of the NIR-T/BSS method emerged after several years of theoretical considerations and model studies dedicated to some aspects of interaction and propagation of near-infrared radiation within tissues of the head, and particularly studies of the fate of NIR beam emitted by the source (emitter, E) into the cranial cavity and the paths of its propagation back to head surface, where it can be received by sensor/s (S) and constitute source of information on the changes of the width of the subarachnoid space. Those theoretical analyses and model studies were focused on two key goals:
1. To explore and elucidate the causes of failure of the earlier attempts to devise a method of assessment of the width of the subarachnoid space in which I also participated (“Encephalovolumeter IR” project by Skalski, Frydrychowski, and Mazur); that concept – assuming such design of the emitter-sensor module in which the E and S were closely adjacent (side by side of each other), proved unsuccessful. As demonstrated in my later studies, the sensor in the old project common with Skalski and Mazur was receiving mainly that part of the beam emitted by the source whose propagation path was contained within the skin and skull bone and not the SAS; for assessment of the width of SAS to be possible it is absolutely necessary that the NIR beam travels from E to S through the SAS. Therefore, the method named “Encephalovolumeter IR” was not meeting the principal a priori requirement. The failure of the “Encephalovolumeter IR” method was the direct reason, why I left the team (Skalski, Frydrychowski, Mazur) and started my own and independent explorations in search of a successful solution of the above-described problem.
2. To attempt a new approach and design a SAS width assessment system, utilizing NIR as information carrier, and building on the knowledge and experience gathered earlier on the causes of failure of the “Encephalovolumeter IR” method; in spite of the failure of the old project I had a strong conviction that building such a system is possible.
Several years spent on analysis of information and reports on the properties of near-infrared radiation and its propagation within human tissues, along with persistent efforts aimed at devising an appropriate, efficient hardware-software system that could enable recording and analysis of signals dependent on long-term and instantaneous changes of the width of SAS were finally concluded with success. This found confirmation not only in the results of experiments on animals and volunteers, which proved coherent and logically followed the knowledge of physiological reactions and regulatory mechanisms, but also in the awards I was appointed for this invention at the international invention and new technology exhibitions in Brussels (1997) and Geneva (1998). Further work on the development of the subsequent versions of increasingly sophisticated prototypes of the system resulted in significant refinement of the quality of the tracings of the transillumination signals (from DS and PS) and their transformations (TQ, cc-TQ, periodograms), which enabled yet more precise assessment of the investigated parameters of intracranial homeostasis. The principles of the system proposed by me and my team after a series of theoretical analyses and model studies contain two essential elements:
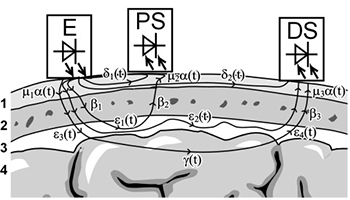
(1) utilization of two sensors located at different separation distances from the NIR source (emitter, E): A – one at the distance of 5-10 mm, referred to as proximal sensor (PS), and B – the other at the distance of 20-30 mm – referred to as the distal sensor (DS)
(2) comparison of the signals recorded from both sensors instead of measuring absolute signal power readings; for relative comparisons of the signals the quotient of the powers of the signals from DS and PS is used, referred to as the transillumination quotient (TQ).
The first of the two elements enables recording of two raw signals generated at the sensors (PS and DS) under the influence of the NIR beams reaching them, propagated within the tissues of the head via different paths; the signal from the distal sensor is modulated by the changes of the width of the natural optical duct constituted by the cerebrospinal-fluid-filled subarachnoid space (SAS). The other element (dividing the power of signal from DS over that of the signal from PS) enables comparison of the two signals with automatic elimination of so-called proportional factors, i.e. those which exhibit the same direction and phase of influence on the individual raw signals from the sensors. These two new elements implemented in the system devised by my team account for the success of the NIR-T/BSS method and make it different from any other application of NIR used for medical purposes. Noteworthy, the only physical variable measured in the NIR-T/BSS method is the power of near-infrared radiation received by the sensors, originating from the NIR source in the form of an electroluminescent diode. The powers of signals generated by each of the sensors depend on the amount of radiation reaching them, and this in turn – similar to the dependence of amount of light propagated within a fiberoptic conductor on its diameter – depends on the width of the optical duct, which for the NIR beam following the deep propagation path from the emitter to the distal sensor (DS) is the cerebrospinal-fluid-filled subarachnoid space (SAS). Increase in the width of SAS results in an increase of the power of the signal from DS and consequently also of the transillumination quotient (TQ) and its sub-cardiac component (scc-TQ), whereas a decrease in the width of SAS leads to a decrease of DS signal power, TQ and scc-TQ. Likewise, the minimum values (valleys) of the pulsatile waveform of the cardiac component of TQ (cc-TQ) are synchronous with minimum instantaneous width of SAS, and its maximum values (peaks) coincide with maximum instantaneous width of that space. Thus, the NIR-T/BSS method consists in recording of signals dependent on short-period (fast-variable) and long-period (slow-variable) oscillations and fluctuations of the width of the subarachnoid space, with all information on the changes of amplitude of cerebrovascular pulsation being derived from this primary input. Model studies have been performed on: 1) samples of human skull bones, scalp and specimens of brain tissue, mechanical-optical model, and mathematical model. Experiments on tissue samples provided data concerning transmittance, reflectance and refraction coefficients for NIR of the examined tissues of the head. Measurements performed in experiments on mechanical-optical model yielded information on the dependence of the power of radiation received by the sensor on the thickness of the skull bone, width of the fluid layer imitating the layer of cerebrospinal fluid within the subarachnoid space, and the emitter-sensor separation distance. Results of mathematical modeling studies provided an insight into the fate of a hypothetical NIR beam propagated within anatomical layers of the head, and helped to assess the influence of such optical phenomena as reflection, absorption and scattering on NIR propagation within those optical centers. Experiments carried out on animals: 1) confirmed the feasibility of recording of transillumination signals in vivo, 2) demonstrated logical dependence of the power of transillumination signal on NIR optical duct (i.e. SAS) – a decrease in width of SAS, regardless of its cause and dynamics – results in a decrease of the amount of radiation reaching the sensor(s), 3) revealed a direct relationship between the increase of amplitude of cerebrovascular pulsation and the increase of cerebral blood flow (measured indirectly through the assessment of blood flow rate in the common carotid artery). Results of experiments performed in volunteers as well as in patients, utilizing interventions and physiological tests exerting well-known and documented influence on the parameters of intracranial homeostasis (e.g. Valsalva manoeuvre, position tilt tests, static handgrip test, breathing with hypercapnic gas mixtures, etc.) revealed a direct relationship between the mean width of SAS and the magnitude of the sub-cardiac component of TQ (scc-TQ), inverse relationships between the amplitude of the cardiac component (cc-TQ) – reflecting the amplitude of cerebrovascular pulsation – and: A. instantaneous arterial blood pressure, and B. instantaneous intracranial pressure, 2) provided information confirming the logic of the changes of the recorded signals and their transformations and consistence of those changes with known regulatory reactions of the cerebral circulation in changing physiological conditions. Summing up, the analyses, studies and experiments confirmed operational consistence of the method of Near InfraRed-Transillumination/Back Scattering Sounding (NIR-T/BSS) with the adopted assumptions and the feasibility of its application for the assessment of vital parameters of intracranial homeostasis and regulatory mechanisms of the cerebral circulation. The information acquired with the NIR-T/BSS method makes this technique a valuable investigational tool for the exploration of physiological mechanisms in healthy volunteers as well as a promising diagnostic modality for: the assessment of the degree and dynamics of impairments of cerebral blood supply, monitoring of changes in SAS width in pre-edema phase in patients with cranio-cerebral injuries, and investigation of the character and degree of vasomotor disorders in patients suffering from different types of headache. Based on the collected knowledge on the theory and functioning of the NIR-T/BSS method, it can be expected that its implementation e.g. in patients with head injuries could facilitate optimized utilization of such diagnostic techniques as computerized tomography (CT) and magnetic resonance imaging (MRI), by both suggesting an important diagnostic moment for a scan to be performed, thus increasing patient safety, and preventing utilization of the CT or MRI scans when it is not necessarily needed (when there are no significant dynamic changes in NIR-T/BSS signals), thus contributing to limitation of the costs of the diagnostic process and monitoring of patient condition. Additional benefits of the method are portable system enabling bedside assessment and monitoring of the patient as well as low cost per patient of the measurements.
NIR-T/BSS Method
SAS Pulsation
Signal power registered with NIRT-T/BSS during diastolic and systolic phase of heart cycle
1 – skin (dots density illustrate the amount of blood in skin);
2 – bone;
3 – SAS (subarachnoid space filled with translucent cerebrospinal fluid);
4 – brain surface.
The black lines represent infrared light propagation.
Sensor band
E - emiter,
PS – proximal sensor,
DS – distal sensor.